

Background
Pediatric patients with pulmonary embolism (PE) suffer from exercise intolerance and dyspnea on exertion, often without right heart dysfunction or pulmonary hypertension - at least at rest. The pathophysiology of the exercise limitation following pediatric PE therefore remains incompletely understood.
Objectives
To extend our understanding of exercise intolerance in pediatric patients with PE by examining ventilatory and hemodynamic responses to exercise.
Methods
To accomplish our goal, we instituted a standardized institutional protocol to systematically assess exercise capacity in pediatric PE patients in the first 3 months following diagnosis. Between February 2019- June 2020, 15 patients underwent resting pulmonary function tests and an incremental symptom-limited cardiopulmonary exercise testing (CPET) to obtain peak exercise in 8-12 minutes. All patients had received anticoagulation for at least 3 months. In all patients, right and left ventricular systolic and/or diastolic dysfunction at rest was ruled out by transthoracic echocardiography. Continuous measurements were made of minute ventilation (VE), oxygen uptake (VO2), carbon dioxide production (VCO2), heart rate (HR), and blood pressure. Predicted values for peak VO2 and work rate were generated from predictive equations. Patients with impaired exercise capacity, defined as <80% of age-, sex- and ideal lean body mass predicted, and dyspnea on exertion underwent further exercise cardiac magnetic resonance (exCMR) imaging using an MR compatible ergometer. Biventricular volumes and contractility, RV longitudinal strain, and RV to pulmonary artery coupling were assessed at rest and with exercise.
Results
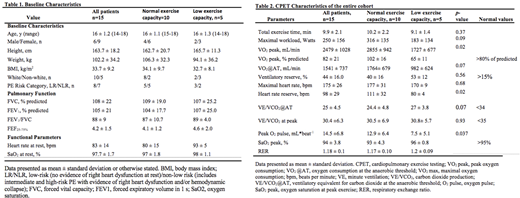
Baseline, clinical characteristics, and CPET data are shown in Tables 1 and 2. Forced Vital Capacity was normal without signs of airway obstruction. Three patients failed to reach their predicted physiologic limits during exercise, and CPET was terminated by the patient prematurely (e.g., muscular exertion, fatigue, & dyspnea, respectively). The mean exercise duration was 9.85 min. The mean ventilatory reserve was within normal limits (>15%) in all but 1 patient. VO2/work rate was normal with normal VO2 at the anaerobic threshold (mean 1541ml/kg/min, SD:731). Exercise capacity, as measured by peak VO2 was reduced, that is, <80% of predicted, in 5 out of the 15 patients (30%). Of these, three patients had echocardiography evidence of RV dysfunction at PE diagnosis, which had resolved at the time of CPET. There were no differences in the mean exercise time and maximal work rate achieved in those with low exercise capacity relative to normal capacity. The ventilatory equivalent for CO2 (VE/VCO2) at peak exercise was elevated (>35) in three of the five patients with decreased exercise capacity. The O2 pulse was attenuated in patients with decreased exercise capacity when compared to those with normal exercise capacity (7.5 mL.beat -1 vs. 12.9-1; p=0.037). Of the two patients who underwent exCMR; one showed reduced right ventricular ejection fraction (38%), abnormal RV strain (-11.3%), elevated right sided pressures signified by interventricular flattening upon inspiration during free breathing scan and an uncoupled RV to the pulmonary circulation.
Conclusions
Reduced exercise capacity is common after PE and not evident by resting evaluations. Pediatric PE patients with low exercise capacity and dyspnea seem to be characterized by either an abnormal pulmonary vascular response to exercise or decreased ventilatory efficiency. Larger studies are needed to better understand exercise pathophysiology after pediatric PE.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal